Rotator Cuff Treatment in Bellingham, WA
Reaching overhead, sleeping on that side, fastening a seatbelt. Rotator cuff problems interfere with basic movement and often persist longer than they should. For tendinopathy and selected partial-thickness tears, PRP, prolotherapy, and shockwave address the tendon directly — with a growing body of evidence supporting their use before surgery is considered.
Book an initial visitCan the rotator cuff heal without surgery?
Bottom line
Most rotator cuff tendinopathy and many partial-thickness tears improve with structured rehabilitation. For chronic pain that persists after several months, PRP is the best-studied regenerative option, with prolotherapy and shockwave as additional choices. Full-thickness tears are a different category and often need surgical evaluation — exam findings and diagnostic ultrasound help clarify which situation you are in.
The rotator cuff is a group of four tendons that stabilize the shoulder and power overhead movement. Rotator cuff problems exist on a continuum: tendinopathy (degeneration and irritation of the tendon), partial-thickness tears (a defect through part of the tendon), and full-thickness tears (all the way through). Pain with reaching, lifting, and sleeping on the shoulder is common across all of them.
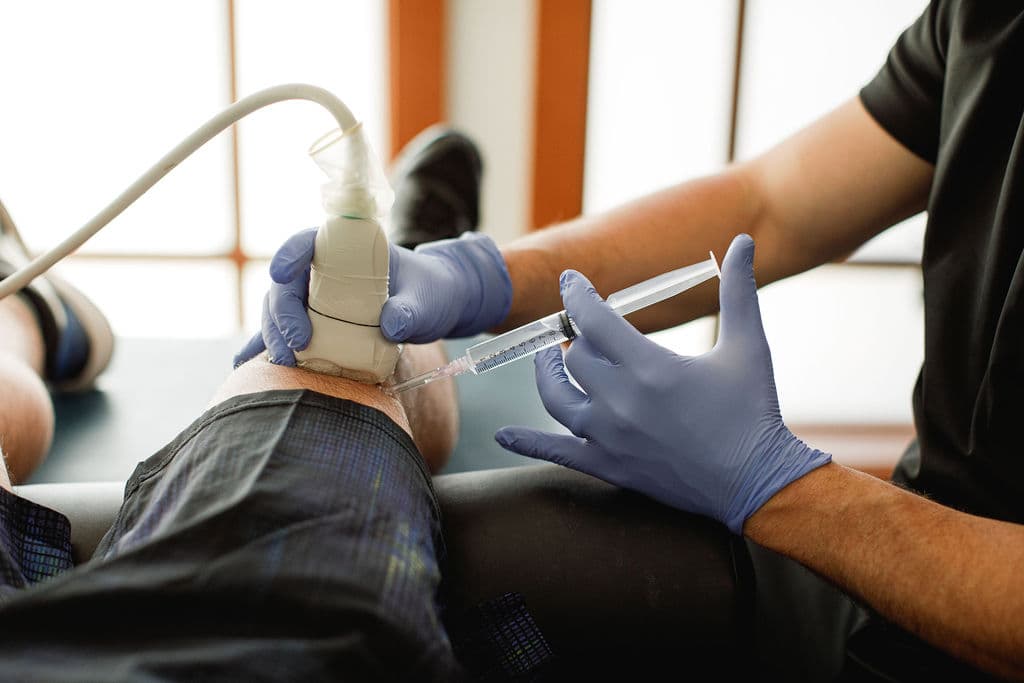
Platelet-Rich Plasma (PRP) therapy concentrates the platelets and growth factors from a small sample of your own blood and delivers them directly into the injured tendon under ultrasound guidance. The goal is to stimulate a genuine healing response in a tendon that, on its own, often heals slowly and incompletely.
Rotator cuff tendinopathy and partial tears are where the PRP evidence is strongest — full-thickness tears and frozen joint presentations are a different clinical question. Ultrasound at the visit helps clarify exactly what is present so the recommendation matches the actual finding.
Rotator cuff tendons that remain in a degenerative state tend not to recover on their own — and repeated cortisone shots, while helpful short-term, can weaken tendon tissue with repeated use. For shoulders that have already tried standard routes, waiting rarely makes the tendon easier to treat.

Your imaging may not tell the whole story
Rotator cuff changes on an MRI are extremely common — and frequently painless. In a 2026 study in JAMA Internal Medicine, researchers scanned 602 randomly selected adults and found that the large majority had at least one rotator cuff abnormality, including a high rate of partial-thickness tears, even though many had no shoulder pain at all. Abnormalities were nearly as common in pain-free shoulders as in painful ones.
A scan finding is not the same as a pain generator.
A finding on a scan doesn't automatically explain your pain or mean you need surgery. What matters is matching treatment to your actual symptoms and how your shoulder functions — which is why Dr. Borys evaluates your shoulder in person, with diagnostic ultrasound, rather than treating an imaging report.
Read the study on PubMedWhy patients consider regenerative rotator cuff care
For chronic rotator cuff problems, these options offer something cortisone doesn't: a way to support healing in the tendon tissue itself.
Reach into a cupboard, sleep on that shoulder, and throw without bracing for the pain
Stay active and working without modifying every movement around a tender shoulder
Potentially delay or avoid surgery when the tendon is still a good candidate — an option that addresses the tissue, not just the pain signal
Break the cortisone cycle — shots that help briefly then fade, leaving the tendon weaker
Accurate ultrasound-guided placement into the exact area of damage
Get a real picture of what your tendon looks like — not just what the MRI report says
Where these treatments fit: conservative care comes first
Injections and shockwave are not the first thing to try for rotator cuff pain. For most people, a structured rehabilitation plan should come first — and many shoulders improve without any procedure.
Rehab is still first — but it has a limit
Structured rotator cuff and scapular strengthening is the right starting point, and many partial tears and tendinopathy cases improve with rehab alone. PRP, prolotherapy, and shockwave earn their place when months of consistent conservative care haven't resolved the pain. If your shoulder has already had a real trial of rehab, activity modification, and perhaps a cortisone shot, continuing to wait tends not to reverse the tendon's condition — it just delays the conversation. Dr. Borys reviews what you've already tried and recommends a next step only when it genuinely makes sense for your shoulder.
Non-surgical options for rotator cuff tendinopathy & partial tears
When conservative care hasn't resolved your shoulder pain, Dr. Borys matches the treatment to your exam findings. PRP is often the first option considered, with prolotherapy and shockwave available when they are a better fit.
PRP Injections
Concentrated platelets and growth factors from your own blood are placed into the injured rotator cuff tendon under ultrasound guidance to support genuine tissue repair. The best-studied regenerative option for rotator cuff tendinopathy and partial tears, which is why it is often considered first.
Learn more about PRP therapyProlotherapy
A dextrose-based solution is injected to prompt a localized healing response in the tendon and surrounding tissue. A gentler regenerative option delivered as a short series, appropriate for selected shoulders.
Learn more about prolotherapyShockwave Therapy (ESWT)
Acoustic pressure waves stimulate blood flow and a healing response in the tendon — with no injection, brief activity modification, and usually no meaningful downtime, with most patients back to light activity the same day. Particularly useful for calcific rotator cuff tendinitis, and an option when a non-injection approach is preferred.
Learn more about shockwave therapyWhat to expect after treatment
Rotator cuff tendons heal slowly. Knowing what the weeks in between look like helps you stay the course.
Soreness at the shoulder
Increased aching or tenderness at the injection site for up to a week is expected — it is the inflammatory response the tendon needs. Overhead work and heavy lifting are restricted. Reduce activity to keep discomfort manageable.
Activity as tolerated: if pain is above a 2 out of 10, ease back. Avoid NSAIDs — the inflammatory cascade is part of what PRP is designed to trigger.
The quiet phase
Initial soreness fades but improvement is not yet clear. The tendon is in early remodeling. Feeling close to baseline without clear progress is normal — this is the phase most likely to feel uncertain.
Light daily activity is usually fine; return to overhead work and resisted movement follows Dr. Borys's specific guidance.
Early improvement
Most patients begin noticing reduced pain with reaching, sleeping on the shoulder, and daily use. Structured rehab — if part of the plan — typically resumes in this window, gradually building load.
Full response window
Tendon effects take 3–4 months to be fully appreciated. Rotator cuff remodeling continues for months beyond that. Dr. Borys reassesses at this point to determine whether the response warrants further treatment.
Patients who combined PRP with prolotherapy may have a slightly different timeline — Dr. Borys will set expectations specific to your case.
Supporting your recovery
Some shoulder soreness is normal
Mild soreness or aching at the shoulder for a few days is expected after an injection and is part of the healing response as the tendon responds to treatment.
Ease back into activity
Heavy lifting and overhead work are usually limited for a short period, after which you progress back into normal use and your rotator cuff rehab on the timeline Dr. Borys lays out for you.
Avoid anti-inflammatories
Unless directed otherwise, avoid NSAIDs (such as ibuprofen) around an injection, since they can blunt the healing response PRP and prolotherapy are meant to support.
Improvement takes time
Rotator cuff treatment works gradually. Many patients notice clearer improvement around 6–12 weeks, with continued change over several months as the tendon heals.
Is this treatment right for your shoulder?
These options can help the right shoulder, but they aren't ideal for everyone. A consultation and exam help determine what fits your situation.
Treatment may be a good fit if you
- Have chronic rotator cuff tendinopathy or a partial-thickness tear that has lasted months
- Have not had lasting relief from physical therapy, activity changes, or other conservative care
- Want a non-surgical option that supports tendon healing
- Can allow several weeks to months for a gradual response
Less likely to be appropriate if you
- Have a brand-new strain that may still respond to rest and rehab
- Have a large full-thickness or complete rotator cuff tear that may need surgical evaluation
- Need immediate or guaranteed pain relief
- Have an active infection, certain blood or platelet disorders, or active cancer (for injection options)
This list is a general guide, not medical advice. Dr. Borys will review your history, exam and goals to recommend the most appropriate option for your shoulder.
If that sounds like your shoulder, it's worth a conversation.
An initial evaluation covers your history, exam, and the options that actually make sense for your tendon.
What the evidence says
These peer-reviewed studies look at PRP, shockwave, and conservative care for rotator cuff tendinopathy and partial-thickness tears — the situations addressed on this page. The evidence is encouraging but still evolving, and no treatment works for every shoulder.
PRP vs Corticosteroid: Durable Benefit
Systematic review and meta-analysis (Yuwarungsikul et al., Knee Surg Sports Traumatol Arthrosc, 2026) finding that PRP provides a modest but durable functional benefit over corticosteroid injection for rotator cuff tendinopathy over longer-term follow-up.
Read on PubMedPRP Added to Physiotherapy for Partial Tears
Clinical study (Demiral et al., Knee Surg Sports Traumatol Arthrosc, 2026) reporting that adding PRP to physiotherapy reduced tear volume and improved functional outcomes in articular-sided partial-thickness supraspinatus tendon tears.
Read on PubMedShockwave for Calcific Tendinitis
Systematic review and network meta-analysis (Yao et al., EFORT Open Rev, 2025) evaluating treatments for rotator cuff calcific tendinitis — one of the strongest indications for shockwave, where it is a well-established non-surgical option alongside needling.
Read on PubMedConservative Treatments Compared
Systematic review and network meta-analysis (Liu et al., Arthroscopy, 2026) finding no significant differences between conservative treatment approaches for partial-thickness rotator cuff tears, supporting structured rehabilitation as the appropriate first step.
Read on PubMedSurgical vs Non-Surgical Therapy
Systematic review and meta-analysis (Ricker et al., BMC Musculoskelet Disord, 2026) comparing surgical and non-surgical therapy for partial rotator cuff tears, supporting a trial of non-surgical care for appropriately selected patients.
Read on PubMedReferences are provided for education and transparency and do not represent a guarantee of any particular outcome. Study populations, PRP and prolotherapy preparations, and shockwave protocols vary, and individual results differ.
Why not just get a cortisone shot?
Cortisone has long been a go-to for shoulder pain. It's a fair question — and the honest answer comes down to short-term relief versus the effect on the tendon itself.
What a cortisone shot does
A corticosteroid injection is anti-inflammatory and can ease shoulder pain quickly. The trade-off is that the relief is often short-lived and the injection doesn't repair the degenerated tendon — so the pain frequently returns.
Why Dr. Borys limits it
There is evidence that repeated steroid injections around the rotator cuff can weaken tendon tissue over time — a particular concern if surgery may eventually be needed. For chronic cases, Dr. Borys favors options that aim to support tendon healing over time.
Rotator cuff treatment — Bellingham, WA
Based in Bellingham, Dr. Borys sees patients from Whatcom County, Skagit County, the San Juan Islands, and surrounding Northwest Washington communities.
Related conditions
Calcific tendinitis
Calcium deposits in the rotator cuff cause a distinct pain pattern — shockwave is the primary non-surgical option and is often more effective than for pure tendinopathy.
Frozen shoulder
Adhesive capsulitis often develops secondary to rotator cuff problems — distinct presentation, different treatment emphasis.
Tennis elbow
Lateral elbow tendinopathy shares the same PRP and shockwave evidence base as rotator cuff tendinopathy.
Rotator Cuff Treatment: Common Questions
Can a partial rotator cuff tear heal without surgery?
Many partial-thickness rotator cuff tears and cases of rotator cuff tendinopathy improve without surgery. The first-line treatment is a structured rehabilitation program — rotator cuff and scapular strengthening, activity modification, and time — and a large share of partial tears improve with this alone.
When pain and weakness persist despite several months of consistent rehab, ultrasound-guided options such as PRP, prolotherapy, or shockwave therapy may be considered to support tendon healing before turning to surgery. Complete (full-thickness) tears are a different situation and often need surgical evaluation. Dr. Borys uses your exam and diagnostic ultrasound to determine which category your shoulder falls into and gives you an honest recommendation.
Does PRP work for rotator cuff tendinopathy and partial tears?
PRP (platelet-rich plasma) concentrates the healing platelets and growth factors from a small sample of your own blood and delivers them, under ultrasound guidance, into the injured rotator cuff tendon to support tissue repair. For rotator cuff tendinopathy and partial-thickness tears, a growing body of randomized evidence suggests PRP can produce meaningful, durable improvement — in some studies offering better medium- and long-term outcomes and lower failure rates than corticosteroid injection, and in partial tears, reducing tear volume when added to physiotherapy.
Results vary between studies, and PRP is not right for every shoulder. It is generally reserved for chronic cases that have not responded to rehabilitation. Dr. Borys gives you an honest assessment of whether PRP is a reasonable option for your rotator cuff.
What is the difference between rotator cuff tendinopathy and a partial tear?
Rotator cuff problems exist on a continuum. Tendinopathy (often called tendinitis) is degeneration and irritation of the tendon without a distinct tear. A partial-thickness tear is a defect that involves only part of the tendon’s thickness, while a full-thickness tear extends all the way through.
Tendinopathy and partial tears share the same patient profile, the same workup, and respond to the same conservative and regenerative options, which is why they are addressed together here. Full-thickness or complete tears are managed differently and often warrant surgical evaluation. Diagnostic ultrasound helps Dr. Borys see where your tendon falls on this spectrum so your treatment is matched to the actual injury.
Are cortisone injections bad for the rotator cuff?
Cortisone (corticosteroid) injections can relieve rotator cuff pain quickly by suppressing inflammation, but the relief is often temporary and the injection does not repair the degenerated tendon. There is also evidence that repeated steroid injections around the rotator cuff can weaken tendon tissue over time, which is a particular concern if surgery may eventually be needed.
For chronic rotator cuff tendinopathy and partial tears, Dr. Borys generally favors treatments that aim to support actual tendon healing — PRP, prolotherapy, and shockwave — rather than relying on repeated cortisone shots.
Do I need surgery for my rotator cuff?
Not necessarily. For rotator cuff tendinopathy and many partial-thickness tears, non-surgical care is a reasonable first approach, and surgery is generally reserved for full-thickness tears, significant loss of function, or shoulders that have not improved after thorough conservative and regenerative treatment.
Non-surgical options such as PRP, prolotherapy, and shockwave aim to support tendon healing without an operation or prolonged recovery. If you have been told you might need rotator cuff surgery, Dr. Borys can give you an honest second opinion on whether non-surgical options are worth trying first based on your exam and ultrasound.
Is rotator cuff treatment covered by insurance in Bellingham?
Regenerative injections such as PRP and prolotherapy, along with shockwave therapy, are generally not covered by insurance and are paid out of pocket, as most plans still classify them as investigational. The initial evaluation, however, is a standard office visit that may be billed through insurance depending on your individual plan and coverage.
Dr. Borys treats chronic rotator cuff pain in Bellingham, WA, serving patients throughout Whatcom County and the surrounding region. Pricing and which option is most appropriate for your shoulder are reviewed at your initial visit.
Been told surgery may be ahead? A second opinion costs nothing.
An initial evaluation starts with an honest assessment of your actual symptoms and exam — what you actually have, what you've tried, and whether a non-surgical path is realistic. That visit is a standard medical evaluation that may be billed through insurance depending on your plan and coverage.